


Colchicine-Macrolide Interaction Risk Calculator
Disclaimer: This tool is for educational purposes only. Always consult your healthcare provider before combining medications. Never adjust doses without professional medical advice.
Step 1: Select Antibiotic
Step 2: Patient Factors
Symptom Checker: Early Signs of Toxicity
Select any symptoms currently experienced (these may indicate early colchicine toxicity):
Nausea
Vomiting
Diarrhea
Abdominal Pain
Unusual Weakness
Dark Urine
You might be treating a gout flare or managing heart inflammation with colchicine, a medication that has saved countless patients from severe pain. At the same time, you might pick up a prescription for a common respiratory infection. It seems harmless enough. But if that antibiotic is a specific type of macrolide, you are walking into a dangerous trap. This combination doesn't just reduce effectiveness; it can trigger life-threatening toxicity. The culprit isn't a random side effect. It is a precise pharmacological clash involving two critical body systems: CYP3A4 enzymes and P-glycoprotein (P-gp) transporters.
The Hidden Mechanism: Why This Combination Fails
To understand why this mix is so dangerous, you need to look at how your body handles colchicine. Colchicine is not like most drugs where a little extra dosage makes no difference. It has an incredibly narrow therapeutic window. This means the dose that works is very close to the dose that harms you. Normally, your liver uses an enzyme called CYP3A4 to break down colchicine before it circulates too widely. Simultaneously, a protein pump known as P-glycoprotein acts as a security guard in your gut and kidneys, pushing any unabsorbed colchicine back out of your cells so it leaves your body.
When you introduce certain macrolide antibiotics into this system, they shut down both safety mechanisms. These drugs inhibit CYP3A4, stopping the breakdown of colchicine. They also block P-glycoprotein, trapping the drug inside your cells. Research published in Rheumatology by Stamp et al. in 2024 highlights that concurrent use of these inhibitors can double plasma concentrations via CYP3A4 inhibition alone. When P-gp is also blocked, concentrations can quadruple. This synergy creates a toxic buildup that standard dosing cannot prevent.
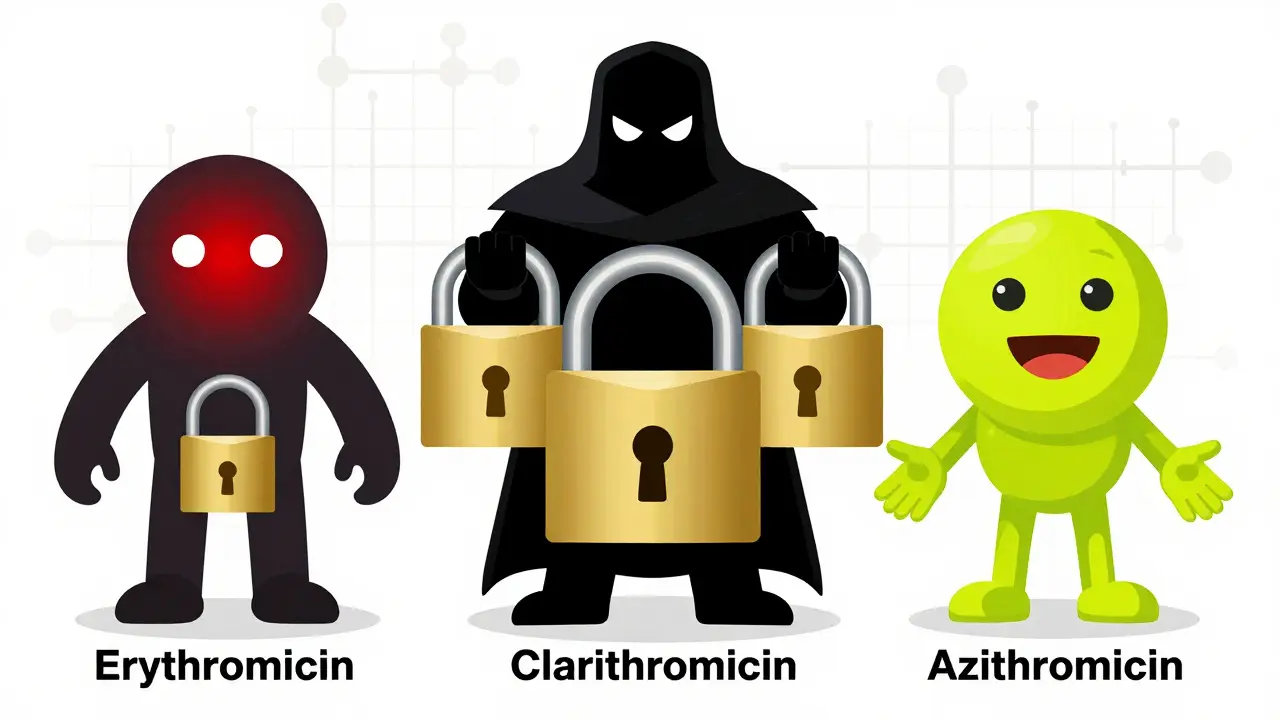
Not All Macrolides Are Equal
A major misconception is that all macrolides carry the same risk. They do not. While they share a similar chemical structure, their ability to inhibit CYP3A4 and P-gp varies drastically. You must distinguish between the high-risk agents and the safer alternatives.
| Antibiotic | CYP3A4 Inhibition | P-gp Inhibition | Clinical Risk Level |
|---|---|---|---|
| Clarithromycin | Strong (IC50 1.6 μM) | Strong (IC50 12.7 μM) | High / Contraindicated |
| Erythromycin | Moderate (Ki 30 μM) | Moderate | Moderate / Use Caution |
| Azithromycin | Minimal | Minimal | Low / Safe Alternative |
Clarithromycin is the most dangerous offender here. It is a potent dual inhibitor. Clinical data shows it poses the highest risk for severe adverse events. Erythromycin is less potent but still significant enough to cause issues, especially in vulnerable patients. On the other hand, Azithromycin barely touches these pathways. A 2022 cohort study by Tan analyzed over 12,000 patients and found that azithromycin demonstrated no clinically significant interaction with colchicine. Switching to azithromycin resolves the vast majority of potential interaction scenarios.
Recognizing the Signs of Toxicity
If this interaction occurs, the symptoms can escalate quickly. Because colchicine affects microtubules in rapidly dividing cells, toxicity manifests in tissues that regenerate fast, such as the bone marrow and gastrointestinal lining. Early signs often include severe nausea, vomiting, and diarrhea. However, these are easily mistaken for typical stomach bugs or side effects of the antibiotics themselves, leading to delayed treatment.
The real danger lies in systemic failure. As colchicine levels rise, you may experience neutropenia, a dangerous drop in white blood cells that leaves you susceptible to infections. More severely, it can cause rhabdomyolysis, where muscle tissue breaks down and releases damaging proteins into the blood, potentially leading to kidney failure. In extreme cases documented in the FDA Adverse Event Reporting System, multi-organ failure and death have occurred. Plasma concentrations exceeding 3.3 ng/mL in patients with renal impairment are particularly hazardous. If you feel unusually weak, notice dark urine, or develop persistent GI distress after starting this combination, seek medical attention immediately.
Who Is Most at Risk?
While anyone can experience this interaction, certain groups face exponentially higher risks. The primary factor is kidney function. Since colchicine is partially excreted by the kidneys, any reduction in renal clearance compounds the problem caused by metabolic inhibition. Elderly patients, who often have reduced kidney function and take multiple medications, are disproportionately affected. Additionally, genetic factors play a role. A 2023 study in Nature Medicine showed that specific genetic polymorphisms, such as the CYP3A5*3/*3 genotype, can predict susceptibility to toxicity. Patients with these genetic markers process colchicine more slowly, making them even more vulnerable when combined with inhibitors.
Other high-risk drugs exacerbate this issue. If you are taking other strong CYP3A4 or P-gp inhibitors alongside colchicine and a macrolide, the risk skyrockets. Common culprits include verapamil, diltiazem, amiodarone, and antifungal agents like ketoconazole or itraconazole. Even some HIV protease inhibitors, such as ritonavir, present greater interaction risks than macrolides due to their extreme potency in inhibiting CYP3A4.
Clinical Management and Safety Protocols
So, what should you do if you need both medications? First, never adjust your doses without consulting your healthcare provider. The American College of Rheumatology explicitly warns against combining colchicine with strong inhibitors like clarithromycin. If avoidance is impossible, strict protocols apply. For moderate inhibitors like erythromycin, guidelines recommend reducing the colchicine dose by at least 50%. Some experts suggest extending the dosing interval significantly.
Therapeutic drug monitoring is ideal but rarely available. Only about 37% of US hospitals have routine access to colchicine level testing. Therefore, clinical vigilance is your best defense. Watch for early signs of toxicity mentioned above. If you are prescribed a macrolide, ask your doctor specifically about switching to azithromycin. It is effective for many common infections and bypasses this metabolic clash entirely. Furthermore, ensure your electronic health records are up to date. Many adverse events occur because specialists are unaware of medications prescribed by general practitioners. Always disclose all supplements and over-the-counter drugs, as some may contain ingredients that affect these pathways.
Future Directions in Safe Treatment
The medical community recognizes this gap in safety. New developments aim to mitigate these risks. Improved clinical decision support systems, such as Epic's updated alert tiers, have reduced inappropriate prescribing by over 60% in recent studies. Researchers are also working on next-generation colchicine analogs. Phase I trials of derivatives like COL-098, which are not substrates for P-gp, show promising results with significantly lower interaction risks. Until these alternatives become widely available, understanding the interplay between colchicine, macrolides, and your body's metabolic guards remains essential for safe care.
Can I take azithromycin with colchicine?
Yes, azithromycin is generally considered safe to take with colchicine. Unlike clarithromycin or erythromycin, azithromycin does not significantly inhibit CYP3A4 or P-glycoprotein, meaning it does not increase colchicine levels in your blood. It is often recommended as the preferred macrolide alternative for patients on colchicine therapy.
What are the symptoms of colchicine toxicity?
Early symptoms include severe nausea, vomiting, abdominal pain, and diarrhea. As toxicity progresses, you may experience neutropenia (low white blood cell count), rhabdomyolysis (muscle breakdown), peripheral neuropathy, and potentially multi-organ failure including kidney and liver damage. Immediate medical attention is required if these symptoms appear.
Why is clarithromycin more dangerous than erythromycin with colchicine?
Clarithromycin is a much stronger inhibitor of both CYP3A4 and P-glycoprotein compared to erythromycin. Its higher potency in blocking these metabolic pathways leads to a more dramatic accumulation of colchicine in the body, resulting in a higher risk of severe toxicity and adverse events.
How does kidney disease affect this interaction?
Kidney disease significantly increases the risk of colchicine toxicity. Since the kidneys help eliminate colchicine from the body, reduced renal function slows down clearance. When combined with drugs that inhibit metabolic breakdown, colchicine levels can reach toxic thresholds much faster, making dose adjustments critical for patients with impaired kidney function.
Are there other drugs besides macrolides that interact with colchicine?
Yes, many drugs inhibit CYP3A4 or P-gp. High-risk combinations include verapamil, diltiazem, amiodarone, ketoconazole, itraconazole, ritonavir, and cyclosporine. Even grapefruit juice can mildly inhibit CYP3A4, though its effect is usually less clinically significant than pharmaceutical inhibitors. Always check for interactions with all new medications.




