Why Your Antifungal Might Not Be Working
If you’re taking a proton pump inhibitor (PPI) like omeprazole or pantoprazole for heartburn-and also an antifungal like itraconazole for a fungal infection-you could be fighting a silent battle inside your stomach. The very drug meant to calm your acid might be quietly starving your antifungal of what it needs to work. This isn’t speculation. It’s documented, measurable, and happening to thousands of people every month.
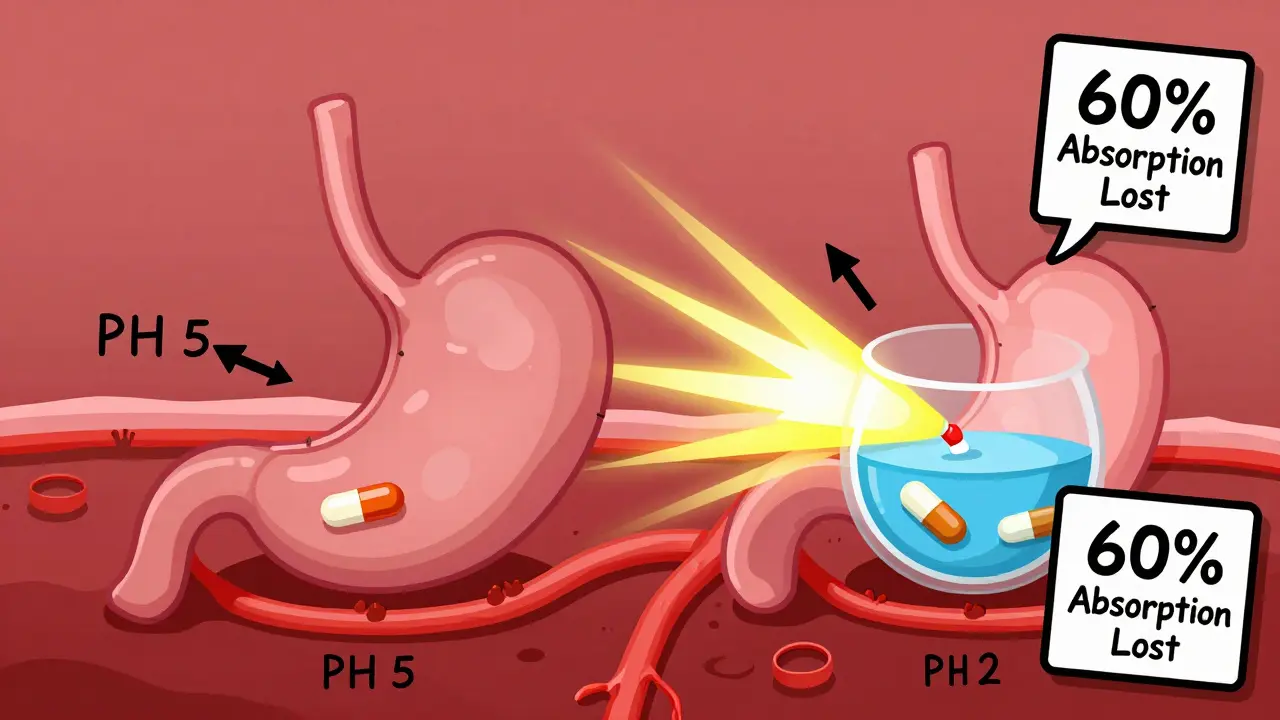
Take itraconazole, one of the most common antifungals used for serious infections like aspergillosis or coccidioidomycosis. It’s a weak base. That means it needs a low pH-below 3-to dissolve properly in your stomach. Without that acidic environment, it just sits there, undissolved, and gets passed through your gut without being absorbed. PPIs raise your stomach pH to 4-6. That’s not just a little change. It’s enough to drop itraconazole absorption by 50-60%. That’s not a minor reduction. That’s treatment failure territory.
The Real Numbers Behind the Interaction
Studies show clear, hard numbers. When omeprazole is taken with itraconazole capsules, the area under the curve (AUC)-a measure of total drug exposure over time-plummets by 60%. That means your body gets less than half the drug it’s supposed to. In one case, a patient with chronic pulmonary aspergillosis had itraconazole levels of just 0.3 mcg/mL. After switching from omeprazole to famotidine, levels jumped to 1.7 mcg/mL. That’s a five-fold increase. And it wasn’t luck. It was physics.
Not all antifungals are affected the same way. Fluconazole? No problem. It’s highly water-soluble and doesn’t care what your stomach pH is. Voriconazole? It takes a hit-about 22% lower exposure with PPIs. Posaconazole delayed-release tablets? Down 40%. But here’s the twist: posaconazole oral suspension doesn’t drop as much. Why? Because it’s already in liquid form. It doesn’t rely on stomach acid to dissolve.
The solution form of itraconazole-liquid, not capsules-also avoids this issue. It’s pre-dissolved. So if you’re on a PPI and need itraconazole, ask your doctor: Can we switch to the solution? That’s not just a workaround. That’s a proven fix.
PPIs vs. H2 Blockers vs. Antacids
Not all acid reducers are created equal. PPIs shut down acid production for 12-24 hours. That’s a long time. H2 blockers like famotidine only last 4-10 hours. Studies show omeprazole cuts itraconazole AUC by 57%. Famotidine? Just 41%. That’s a big difference.
Antacids? They work fast but don’t last. If you take Tums or Maalox two hours before or after your antifungal, the impact is minimal. The timing matters. PPIs? They’re a constant background hum of high pH. You can’t time around them.
So if you need acid suppression while on a pH-sensitive antifungal, H2 blockers are your better bet. But even then, give it a 10-hour window after your antifungal dose. Don’t just take them together.
What About Newer Formulations?
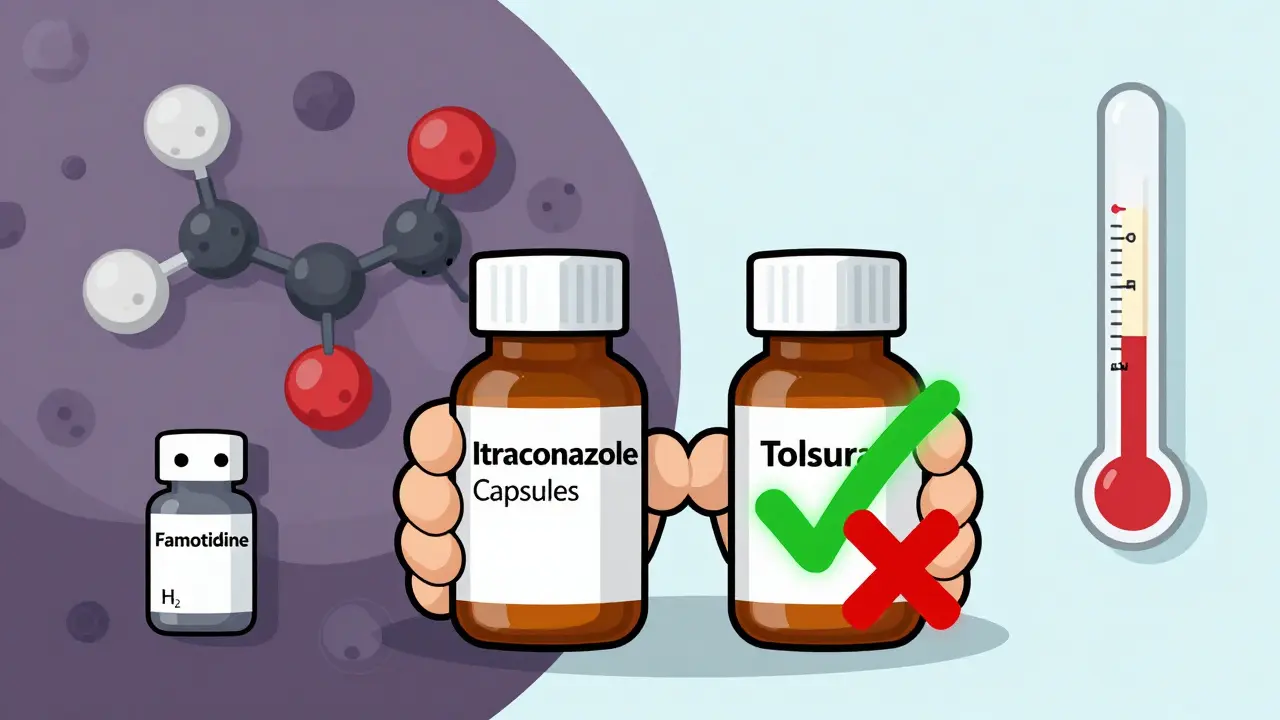
There’s good news on the horizon. In 2023, the FDA approved a new version of itraconazole called Tolsura. Unlike the old capsules, it’s designed to absorb without needing stomach acid. With PPIs, its absorption drops by only 8%-not 60%. That’s a game-changer.
For patients who’ve had multiple treatment failures or are on long-term PPIs, Tolsura is now the preferred option. It’s not cheap, but it’s worth it if your life depends on this drug working. Ask your pharmacist: Is Tolsura an option for you?
The Hidden Risk: Subtherapeutic Levels Create Resistance
Here’s the scary part. If your antifungal levels are too low, you’re not just failing treatment-you’re breeding resistance.
The European Committee on Antimicrobial Susceptibility Testing (EUCAST) warned in 2021 that low drug concentrations from PPI interactions can turn a susceptible fungal strain into a resistant one. That means the fungus survives, mutates, and comes back stronger. Now you need a stronger drug. Maybe one with more side effects. Maybe one that’s more expensive. Maybe one that doesn’t even exist yet.
This isn’t theoretical. There are documented cases where patients with invasive aspergillosis failed treatment because their itraconazole levels were too low-due to PPIs-and later developed resistant strains. That’s not just a drug interaction. That’s a public health concern.
What Can You Actually Do?
Here’s your action plan:
- Check your antifungal. Is it itraconazole capsules? Posaconazole delayed-release tablets? Voriconazole? These are the ones at risk.
- Check your acid reducer. Are you on omeprazole, esomeprazole, lansoprazole, pantoprazole? If yes, you need to act.
- Don’t stop your PPI without talking to your doctor. If you’re on a PPI for a bleeding ulcer or severe GERD, stopping it could be dangerous.
- Ask about switching to the itraconazole solution or Tolsura. These avoid the interaction entirely.
- Ask about switching to famotidine. If you still need acid suppression, H2 blockers are safer.
- Ask about therapeutic drug monitoring. For itraconazole, levels should be 0.5-1.0 mcg/mL. If you’re below that, your dose isn’t working.
One hospital pharmacist in Massachusetts reported that 68% of pharmacists see at least one of these interactions every month. That’s not rare. That’s routine. And too often, it’s missed.

The Unexpected Twist: Could PPIs Help?
Here’s where it gets weird. In a 2025 lab study, researchers found that when omeprazole and itraconazole were mixed together in a petri dish, they killed 77.6% of resistant fungal strains-even those that had survived other antifungals. The same combo worked against azole-resistant Aspergillus fumigatus.
That’s not a mistake. That’s synergy. The same mechanism that blocks absorption in the gut might be enhancing antifungal action in the bloodstream. Researchers at the NIH are now testing low-dose omeprazole with subtherapeutic itraconazole in early-phase clinical trials (NCT05678901). If this works, we might be looking at a new way to treat resistant fungal infections.
But don’t try this at home. This is still experimental. The dose, timing, and patient selection are being carefully studied. What we know for sure is that taking your PPI and antifungal together at random won’t help. It’ll just make things worse.
Who’s at Risk?
You’re more likely to face this interaction if:
- You’re over 65 (PPI use jumps sharply after 60)
- You’re hospitalized (5-7% of inpatients get systemic antifungals)
- You have cancer, HIV, or are on immunosuppressants
- You’ve been on a PPI for more than 3 months
- You’ve had a fungal infection that didn’t improve
Medicare data shows 38.7% of patients prescribed itraconazole capsules also got a PPI in the same month. Only 12.3% of those on itraconazole solution did. That gap tells you something: some doctors know. But many don’t.
The Bottom Line
This interaction isn’t a footnote. It’s a major clinical problem. It costs the U.S. healthcare system $287 million a year in wasted drugs and failed treatments. It leads to hospital readmissions. It creates drug-resistant fungi. And it’s often invisible-because no one checks.
If you’re on a PPI and an antifungal, ask these questions:
- Is my antifungal affected by stomach acid?
- Is there a version of this drug that doesn’t need acid to work?
- Can I switch to famotidine instead of my PPI?
- Can we check my drug levels?
Don’t assume your doctor knows. Don’t assume your pharmacist caught it. This interaction is so common, it’s almost expected. But that doesn’t make it okay. It makes it urgent.
One simple change-switching from itraconazole capsules to the solution, or from omeprazole to famotidine-could mean the difference between recovery and relapse. Don’t wait for a failure to happen. Ask now.
Can I take omeprazole and itraconazole together?
No, not if you’re using itraconazole capsules. Taking them together can reduce itraconazole absorption by up to 60%, making the drug ineffective. If you must take both, switch to the itraconazole solution or Tolsura-these formulations aren’t affected by stomach pH. If you need acid control, use famotidine instead of omeprazole, and take it at least 10 hours after your antifungal.
Does fluconazole interact with PPIs?
No. Fluconazole is highly water-soluble and doesn’t rely on stomach acid for absorption. It works just as well whether you’re on omeprazole, pantoprazole, or nothing at all. You can take fluconazole with a PPI without worrying about reduced effectiveness.
Why does itraconazole need stomach acid to work?
Itraconazole is a weak base. That means it dissolves best in an acidic environment (pH below 3). PPIs raise stomach pH to 4-6, which prevents the drug from dissolving properly. If it doesn’t dissolve, your body can’t absorb it. That’s why capsules fail-but the liquid solution, which is already dissolved, still works.
What’s the difference between itraconazole capsules and solution?
Itraconazole capsules require stomach acid to dissolve and release the drug. The solution is already in liquid form and doesn’t need acid. With PPIs, capsules lose 50-60% of their absorption. The solution only loses 10-15%. That’s why the solution is preferred when PPIs are needed.
Can PPIs make fungal infections worse?
Yes, indirectly. By lowering antifungal drug levels, PPIs can cause treatment failure. That lets the fungus survive and possibly develop resistance. Once resistant, the infection becomes harder-or impossible-to treat with standard drugs. This is why experts warn that PPIs can turn a treatable infection into a life-threatening one.
Should I stop my PPI if I need an antifungal?
Don’t stop it on your own. If you’re on a PPI for a serious condition like a bleeding ulcer or Barrett’s esophagus, stopping it could be dangerous. Instead, talk to your doctor about switching to an antifungal that doesn’t need acid (like fluconazole or itraconazole solution) or switching your acid reducer to famotidine. Your doctor can weigh the risks of stopping the PPI versus the risk of antifungal failure.
Is there a new antifungal that doesn’t interact with PPIs?
Yes. Tolsura, a newer form of itraconazole approved in 2023, is designed to absorb without needing stomach acid. With PPIs, its absorption drops by only 8%, compared to 60% for regular capsules. If you’re on long-term PPI therapy and need itraconazole, Tolsura is now the preferred option.





10 Comments
Okay but real talk-how many people are out there taking omeprazole like it’s candy and then wondering why their yeast infection won’t go away? I had a friend who was on PPIs for 3 years for ‘mild heartburn’ and then got hit with invasive aspergillosis. Turns out her itraconazole levels were practically zero. She didn’t even know the two could clash. This isn’t niche. It’s a silent epidemic.
And don’t get me started on how doctors just assume ‘antifungal’ means fluconazole. Like, nope. Some of us need the heavy artillery. And if you’re on a PPI, you’re basically sabotaging your own treatment unless you ask the right questions.
Oh here we go again with the ‘PPIs are evil’ narrative. Let me guess-you also think antibiotics cause autism and fluoride is a government mind-control plot? The fact that you’re treating a 60% absorption drop like it’s a death sentence is hilarious. People have been taking itraconazole with PPIs for decades and not all of them died. And now you want us to switch to famotidine like it’s some magical elixir? Please.
Also, Tolsura? That’s a $12,000/month drug. Most people can’t even get their insurance to cover the generic. So yeah, let’s just tell everyone to ‘ask their doctor’ while ignoring the real issue: American healthcare is a money-driven circus.
Let me paint you a picture: imagine you’re a 72-year-old with GERD, diabetes, and a history of fungal pneumonia. You’re on omeprazole because your GI doc said ‘it’s safe long-term.’ Then you get hit with aspergillosis. Your pulmonologist prescribes itraconazole capsules. You take them. Nothing happens. Two months later, you’re back in the hospital. Why? Because no one ever connected the dots. Not the pharmacist. Not the nurse. Not even the damn discharge summary.
And now you’re telling me the solution is to ‘switch to the solution’? That’s not a fix-that’s a linguistic joke. The liquid form costs triple, requires refrigeration, tastes like motor oil, and requires you to take it on an empty stomach. Meanwhile, your PPI is still there, silently poisoning your treatment.
Here’s what’s really broken: we treat drugs like isolated entities, not as parts of a biological ecosystem. Your stomach isn’t a test tube. It’s a living, breathing, acid-producing organ that’s been chemically neutered. And we’re surprised when the drugs don’t work?
And don’t even get me started on the fact that 38.7% of patients on itraconazole are also on PPIs. That’s not a coincidence. That’s systemic negligence. Someone’s getting paid to keep this going. Probably someone in a lab coat with a fancy title.
I’ve seen it. I’ve documented it. I’ve fought with pharmacies over this. And the saddest part? The patients never know. They just think they’re ‘not responding to treatment.’ Like it’s their fault. Like they didn’t take it ‘right.’
Meanwhile, the NIH is running trials to see if omeprazole can *enhance* antifungal activity in vitro. So the same drug that’s killing your absorption might be your salvation in a petri dish. Welcome to pharmacology, folks. It’s not science. It’s a soap opera written by chemists with too much caffeine and too little sleep.
Hey everyone-just wanted to say this post saved my mom’s life. She was on omeprazole for years, got a fungal lung infection, and kept getting worse. Her doctor kept upping the antifungal dose. Turns out her levels were way too low. We switched her to famotidine and the itraconazole solution. Within 3 weeks, she was breathing better. No magic, just science.
If you’re reading this and you’re on a PPI + antifungal? Talk to your pharmacist. They’re the real heroes here. Don’t wait for a crisis. Ask now. ❤️
Fluconazole is fine with PPIs. That’s all I needed to know.
Wow this is so helpful 😊 I’ve been on itraconazole for a while and my stomach’s been acting up-I didn’t realize it could be the PPI! Gonna talk to my doc about switching to famotidine. Thanks for breaking it down so clearly! 🙌
The clinical implications of pharmacokinetic interference between proton pump inhibitors and azole antifungals represent a significant, yet underappreciated, therapeutic challenge in modern medical practice. The data presented, while compelling, must be contextualized within the broader framework of evidence-based pharmacotherapy and individualized patient management. The assertion that this interaction constitutes a ‘public health concern’ is not without merit, yet it risks oversimplification of a complex polypharmacy landscape.
Moreover, the recommendation to substitute famotidine for PPIs without consideration of underlying etiology-such as erosive esophagitis or Barrett’s metaplasia-may introduce unintended clinical risks. The proposed ‘action plan’ lacks nuance regarding the risk-benefit calculus inherent in chronic acid suppression.
It is also noteworthy that the 2025 in vitro synergy between omeprazole and itraconazole, while intriguing, remains preliminary and lacks clinical validation. Extrapolation of petri dish results to human therapeutics constitutes a classic case of ecological fallacy.
That said, the call for therapeutic drug monitoring is both prudent and overdue. The integration of pharmacokinetic assays into routine antifungal management protocols warrants serious consideration by clinical pharmacy services.
Let’s be real-this isn’t about science. This is about pharma’s billion-dollar game of musical pills. Omeprazole? Generic. Itraconazole capsules? Generic. But Tolsura? Oh no, that’s the ‘premium’ version. $12,000 a month. Who’s getting rich here?
And don’t tell me about ‘patient safety.’ If this interaction was truly a crisis, the FDA would’ve mandated black box warnings years ago. But they didn’t. Because the PPI market is too big. Because the antifungal market is too small.
Meanwhile, doctors are too busy chasing KPIs to read a 10-page pharmacology paper. And patients? They’re too tired to ask. So we keep doing the same thing and expecting different results.
And now we’re supposed to be impressed that a lab study found a synergy in a petri dish? That’s not innovation. That’s a desperate Hail Mary from researchers who can’t get funding for anything else.
Real solution? Ban PPIs over-the-counter. Make pharmacists screen for interactions before dispensing. Force EHRs to flag these combos. But no-let’s just hand out pamphlets and hope someone reads them.
So now we’re blaming American medicine for this? What about India? They give out PPIs like candy there. And antifungals? Over-the-counter in 90% of pharmacies. You think this problem is just in the US? Wake up. This is a global failure of basic healthcare education.
And don’t even get me started on the ‘switch to famotidine’ crowd. That’s a Band-Aid. The real problem? People think ‘heartburn’ means ‘I ate too much pizza.’ No. It’s often a sign of something deeper. And treating symptoms without diagnosing causes? That’s how you get a nation of zombies on PPIs.
Stop blaming the drugs. Start blaming the system that lets people self-diagnose with Google and then demand a prescription.
And now I see what happened. Nathan King, the pretentious elitist, just dropped his academic bomb and thinks he’s above the rest of us. But here’s the thing-he’s right about one thing: this isn’t just about drugs. It’s about systems.
But he missed the point. We’re not here to write a journal article. We’re here because real people are dying because no one told them to ask about drug levels.
So yeah, your ‘ecological fallacy’ jab is cute. But your ‘prudent’ recommendation for therapeutic drug monitoring? That’s a luxury most patients can’t afford. You’re talking about a $500 blood test while people are choosing between insulin and rent.
Meanwhile, Mandy’s mom got better because someone *asked*. That’s the real win. Not your fancy words. Not your citations. Just someone who cared enough to look beyond the script.
So maybe instead of lecturing us on ‘nuance,’ you could ask: ‘How do we make this simple for the 99% of people who don’t have a clinical pharmacist on speed dial?’
Because if your solution requires a PhD to understand, it’s not a solution. It’s a privilege.