

Apfel Score Calculator for Postoperative Nausea Risk
Patient Risk Assessment
The Apfel score helps determine appropriate antiemetic prophylaxis based on four key risk factors. Each 'yes' adds one point to your total risk score.
Results
Your Apfel Score: 0
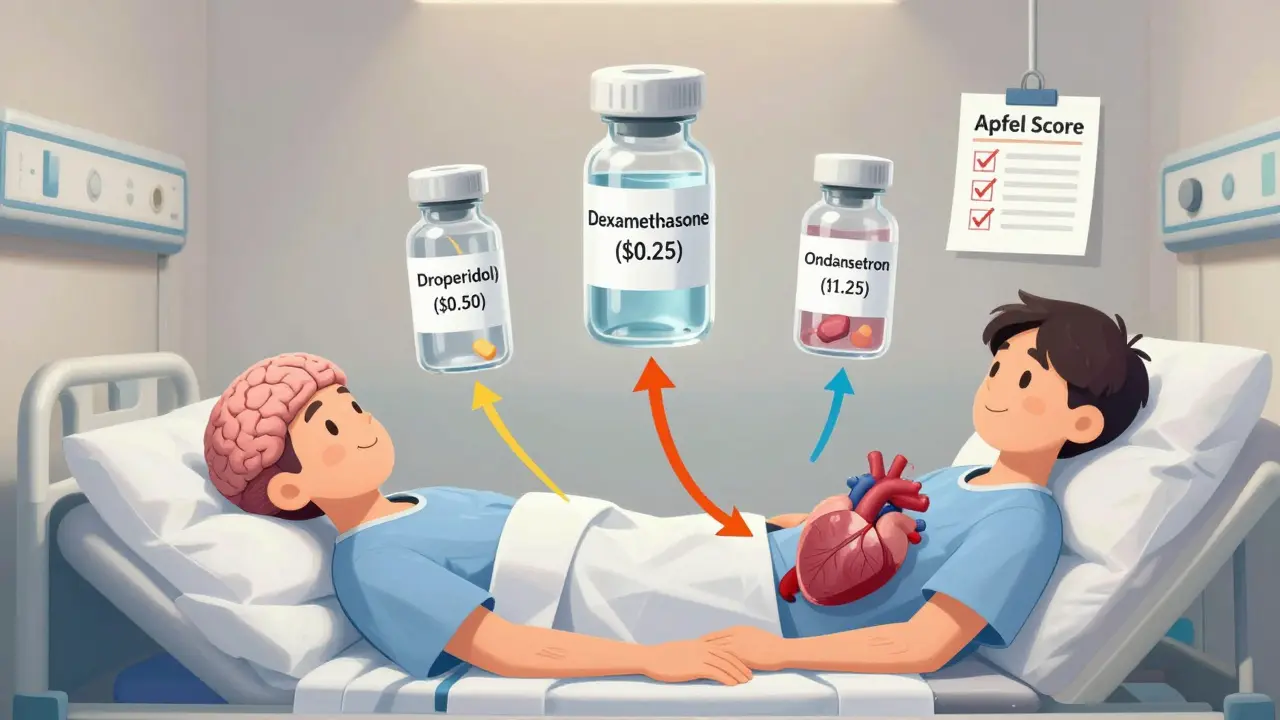
Recommended Drug Options
| Drug | Cost per Dose | Key Benefits |
|---|---|---|
| Droperidol | $0.50 | Fast-acting for opioid-induced nausea; better than ondansetron for many patients |
| Dexamethasone | $0.25 | Boosts effectiveness of other antiemetics by 20-30%; best as add-on |
| Ondansetron | $1.25 | Effective for non-opioid related nausea; avoid if heart conditions present |
When a patient feels nauseous after surgery, chemotherapy, or even a simple painkiller, it’s not just uncomfortable-it can delay recovery, increase hospital stays, and cost thousands in extra care. Medication-induced nausea is one of the most common side effects in modern medicine, yet many clinicians still choose antiemetics based on habit, not evidence. The truth? Not all anti-nausea drugs work the same, and picking the wrong one can mean wasted money, unnecessary side effects, or even dangerous heart rhythms.
Why Some Antiemetics Work Better Than Others
There are seven main classes of antiemetics, each targeting different parts of the body’s nausea pathways. The most common ones you’ll see in hospitals are 5-HT3 antagonists (like ondansetron), dopamine blockers (like droperidol and metoclopramide), and corticosteroids (like dexamethasone). But here’s what most people miss: ondansetron isn’t always the best choice.
It’s true that ondansetron blocks serotonin receptors and stops nausea in about 65-75% of surgical patients. But in opioid-induced nausea-common after pain meds-it’s less effective. A 2023 study of 6,665 cesarean section patients found that combining dexamethasone with ondansetron reduced rescue doses by 32% compared to ondansetron alone. That’s a big deal. One drug isn’t enough when multiple systems are triggering nausea.
Droperidol, on the other hand, blocks dopamine receptors and works faster. In one trial, only 12.1% of patients given 0.625 mg of droperidol had nausea, compared to 21.1% in the control group. And at $0.50 per dose, it’s cheaper than ondansetron’s $1.25. Anesthesiologists on Reddit and hospital forums consistently report it works better for opioid-tolerant patients, with less sedation and fewer headaches.
When Dexamethasone Makes a Difference
Dexamethasone doesn’t block nausea directly. It works slowly-4 to 5 hours-so it’s not for immediate relief. But as an add-on, it boosts the success rate of other antiemetics by 20-30%. That’s not a small bump. In fact, for high-risk patients (those with two or more risk factors), guidelines now recommend pairing it with droperidol. It’s not a magic bullet, but it’s one of the few drugs with solid data for non-chemotherapy cases.
Still, there’s controversy. The OHSU Drug Effectiveness Review Project found weak evidence for dexamethasone outside of cancer care. Yet hospitals keep using it. Why? Because in practice, it works. A 2023 quality improvement project at Massachusetts General Hospital showed a 32% drop in rescue meds when dexamethasone was added to ondansetron. Real-world results often beat clinical trial numbers.
The Hidden Dangers of Popular Choices
Not all antiemetics are safe for everyone. Ondansetron has a black box warning from the FDA for QT prolongation-a heart rhythm issue that can lead to sudden death. This isn’t rare. In one trial, 3% of patients with pre-existing heart conditions had dangerous changes in their ECG after ondansetron. That’s why some hospitals now avoid it in older adults or those on other heart meds.
Metoclopramide (Reglan) has its own risks. At doses over 300 mg per week, it can cause irreversible movement disorders. One ER doctor reported 8% of elderly patients developed severe restlessness (akathisia) after just 10 mg. That’s why many now switch to olanzapine, an antipsychotic with anti-nausea effects, for older patients. It’s not FDA-approved for nausea, but it’s becoming standard in geriatric care.
And then there’s promethazine. It’s cheap. It’s common. But it’s also linked to tissue death if given IV incorrectly. The FDA has issued warnings about its use in children and its risk of severe reactions. Many hospitals have banned it for routine use.

How to Pick the Right One: The Apfel Score
The key to choosing safely isn’t guesswork-it’s risk stratification. The Apfel score, validated in over 20,000 patients, gives you four simple questions:
- Is the patient female?
- Are they a non-smoker?
- Do they have a history of motion sickness or past nausea after surgery?
- Will they get opioids after surgery?
Each ‘yes’ adds one point. Zero to one point? Skip prophylaxis. Two points? Use one drug-either droperidol 0.625 mg or ondansetron 4 mg. Three or four points? Use two drugs: droperidol plus dexamethasone. This isn’t theory. Hospitals that use this system cut PONV rates by half.
And cost? Droperidol at $0.50, dexamethasone at $0.25, and generic ondansetron at $1.25. Compare that to newer combo drugs like Akynzeo, which costs $350 per dose. Most patients don’t need the expensive ones.
What About Newer Options?
There are new drugs on the market. Intranasal ondansetron works fast and avoids swallowing issues. Netupitant/palonosetron (Akynzeo) is great for chemotherapy-75% success rate. But for general surgery? Overkill. These drugs are designed for extreme cases: cancer patients, repeated vomiting, or when older drugs fail.
The future is precision. Researchers are starting to test genetic differences. Some people metabolize ondansetron too fast or too slow because of their CYP2D6 gene. That’s why one patient gets relief and another doesn’t. But right now, that’s still research. For now, stick to the proven, low-cost, risk-based approach.
What Clinicians Are Saying
On Medscape, one ER doctor wrote: "We switched from metoclopramide to olanzapine for elderly patients. Akathisia dropped from 8% to under 1%." Another anesthesiologist on the Society of Critical Care Medicine forums said: "We started using droperidol for all moderate-risk patients. Rescue meds went down 40%. We saved $18,000 in three months."
Meanwhile, patient reviews on Drugs.com show ondansetron works fast-"within 15 minutes"-but 32% report headaches. That’s a trade-off. Droperidol? Fewer side effects, but some fear it because of old warnings. Those warnings were for high doses. At 0.625 mg, it’s safe, effective, and cheap.
Bottom Line: Less Is More
Choosing antiemetics isn’t about using the newest, fanciest drug. It’s about matching the right tool to the right patient. Most people don’t need more than one drug. Most don’t even need that. Use the Apfel score. Avoid promethazine and high-dose metoclopramide. Choose droperidol for moderate risk. Add dexamethasone for high risk. Skip ondansetron if the patient has heart issues. Save the expensive combos for cancer.
The goal isn’t to prevent every single case of nausea. It’s to prevent the cases that matter-those that delay recovery, increase costs, or cause harm. Do that, and you’re doing better than 70% of hospitals.
What’s the most cost-effective antiemetic for postoperative nausea?
Droperidol at 0.625 mg costs about $0.50 per dose and has proven efficacy in preventing nausea after surgery. Combined with dexamethasone ($0.25 per dose), it’s far cheaper than ondansetron ($1.25) and more effective in many cases, especially for opioid-induced nausea. Studies show it reduces rescue medication needs and hospital costs.
Is ondansetron safe for everyone?
No. Ondansetron carries a black box warning from the FDA for QT prolongation, which can lead to dangerous heart rhythms. It should be avoided in patients with existing heart conditions, those taking other QT-prolonging drugs, or those with electrolyte imbalances. For these patients, droperidol or dexamethasone are safer alternatives.
Why is dexamethasone used if it takes hours to work?
Dexamethasone doesn’t work fast, but it enhances the effect of other antiemetics. When given 30-60 minutes before surgery, it reduces nausea for up to 24 hours. It’s not used alone for immediate relief, but as an add-on to ondansetron or droperidol, it improves success rates by 20-30%. It’s especially useful for high-risk patients.
Can metoclopramide cause movement disorders?
Yes. Long-term or high-dose use of metoclopramide (over 300 mg per week) can lead to irreversible movement disorders called tardive dyskinesia. Even at standard doses, it can cause acute restlessness (akathisia), especially in elderly patients. Many hospitals now avoid it in older adults and use olanzapine instead.
How do I know if my patient is at risk for PONV?
Use the Apfel score: 1 point each for female sex, non-smoking status, history of motion sickness or past PONV, and postoperative opioid use. Zero to one point = no prophylaxis. Two points = single antiemetic. Three or four points = dual therapy (e.g., droperidol + dexamethasone). This simple tool reduces unnecessary drug use and improves outcomes.





15 Comments
Ondansetron is overused. I've seen patients throw up anyway and then get a headache on top of it. Droperidol at 0.625 mg? That's the real MVP. Cheap, fast, and no one's getting weird heart vibes. 🤷♀️
Thank you for this meticulously referenced and clinically grounded overview. The Apfel score is not merely a tool-it is a paradigm shift in perioperative care. Evidence-based, cost-conscious, and patient-centered. This should be mandatory reading for all residents.
I work in a trauma center and we switched to droperidol + dexamethasone two years ago. Rescue meds dropped 52%. Ondansetron? We only use it now if the patient specifically asks for it-like they’re ordering a latte. Also, metoclopramide is basically a time bomb for elderly folks. Just say no.
Dude, I used to be all about ondansetron till I saw a 78yo lady get akathisia from 10mg of Reglan. Scary stuff. We switched to olanzapine 5mg and her restlessness went from ‘I’m gonna run outta here’ to ‘I’m fine, thanks’. Also, dexamethasone is like the secret sauce. Not flashy, but it works. 🙌
EVERYTHING YOU’RE SAYING IS RIGHT-BUT WHY ISN’T THE FDA DOING MORE?! THEY LET ONDANSETRON STAY ON THE MARKET WITH A BLACK BOX WARNING AND THEN LET HOSPITALS USE IT LIKE IT’S WATER?! AND PROMETHAZINE?! IT’S A TISSUE KILLER! SOMEONE’S MAKING MONEY OFF THIS! SOMEONE’S PROFITING FROM PATIENT SUFFERING! THIS ISN’T MEDICINE-IT’S A CORPORATE GAME! 🚨💔
They’re hiding the truth. Dexamethasone? It’s not just for nausea. It’s a steroid. And steroids? They’re linked to suppressed immune response. They’re using it because it’s cheap… but what’s the long-term cost? Are we just delaying the real problem? Who funds these studies? Ask yourself.
You're all just repeating hospital pamphlets. Droperidol? Yeah, it works. But you’re ignoring the 2018 FDA advisory on QT prolongation with droperidol too. You think 0.625 mg is safe? That’s what they said about thalidomide too. And dexamethasone? It’s a gateway drug to adrenal suppression. You’re all just lazy clinicians who don’t want to think.
In the grand tapestry of human suffering, nausea is but a thread. Yet we treat it as if it were the loom itself. The body is not a machine to be fixed with pills. The mind, the spirit, the silence between breaths-these are the true healers. A single dose of droperidol may silence the stomach, but it cannot quiet the soul's echo. What is recovery if not the return to harmony? Not dosage. Not cost. Not protocol. But presence.
Droperidol = 💯. Ondansetron = 💀. Dexamethasone = 🤫 (silent but deadly effective). And yeah, promethazine? That’s basically injecting napalm. I’ve seen nurses get sued over it. We banned it here. No regrets. Also, olanzapine for elderly? Game changer. My grandma’s ER doc switched her and she stopped pacing like a zombie. 🧠💤
I love how simple this is. Apfel score = 2? One drug. 3 or 4? Two. No overkill. No guesswork. I wish more places did this. We still have people getting three antiemetics because ‘better safe than sorry’. Nope. Less is more. And droperidol is cheaper than my morning coffee. 🤓
This made me feel seen. I work in oncology and we use Akynzeo all the time… but then I see post-op patients getting the same $350 drug for mild nausea. It breaks my heart. We don’t need fancy when simple works. Thank you for saying what needs to be said.
I’ve been using the Apfel score for 8 years now. It’s not glamorous, but it’s reliable. We’ve cut our antiemetic costs by 60% and improved patient satisfaction. The best part? Nurses don’t have to guess anymore. It’s like having a GPS for nausea. Highly recommend.
Funny how we’ve forgotten that medicine used to be simpler. Before the marketing reps, before the formularies, before the $350 combos… we had clinical judgment. Droperidol and dexamethasone? They’re not new. They’re just forgotten. Sometimes the future is just the past, repackaged.
The ethical imperative here is not merely efficacy-it is proportionality. To administer a drug with a black box warning for a condition that may resolve spontaneously, absent risk stratification, constitutes a form of therapeutic overreach. The Apfel score restores balance. It is not merely clinical-it is moral.
I just want to say-this is the kind of post that makes me proud to be a nurse. You didn’t just list facts. You gave us a framework. A way to think. A way to care. And you did it without jargon. Thank you. 💙